The pitch shows up first on a forum, then in a targeted ad, then, if you spend enough time reading about lifting, everywhere at once. Muscle peptides, the promise goes, are the next quiet edge: a vial, a small needle, a body that recovers faster and holds onto more lean mass than diet and training alone can manage. The compounds have real pharmacology behind them. The marketing, though, got out ahead of the evidence years ago, and the gap between the two is where most people run into trouble.
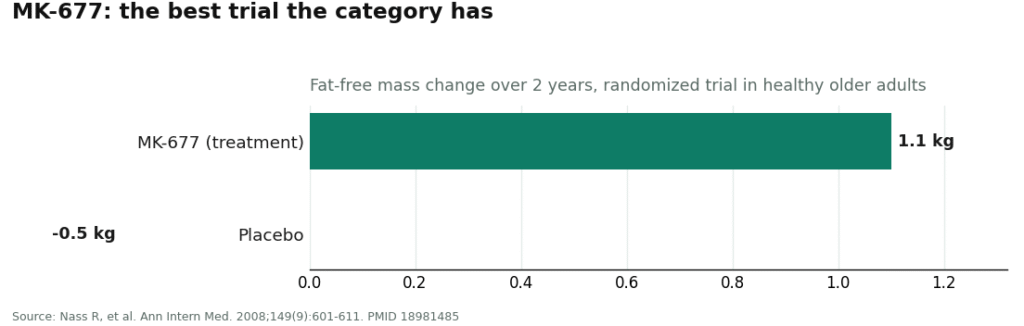
Start with the one number that should color everything else here, because it is the best data the category has to offer. MK-677, the most rigorously studied of the bunch, was tracked in a two-year randomized trial in healthy older adults. It nudged lean mass up by roughly 1.1 kg. But the researchers were blunt about what that gain amounted to: it “did not result in changes in strength or function” [1]. That is the headline result from the best-designed study in the entire field. Everything sold as a shortcut to a better physique sits somewhere south of that modest finding.
So the honest starting point is not “does this work,” exactly. It is “how much of what you’re being told matches what the trials actually found.” That question turns out to be a decent filter for telling apart the providers worth your time from the ones just trying to close a sale. Below are seven ways to run that filter yourself, followed by a plain scorecard of how the major players in this space actually answer them.
How the market split in two
Somewhere along the way, the muscle peptide trade forked into two entirely different businesses that happen to sell overlapping molecules. One branch runs through licensed telehealth: a clinician reviews your history, a licensed pharmacy compounds the product, and everyone involved can be held to a professional standard. The other branch is the research-chemical trade, websites that ship vials labeled “not for human consumption” with no clinician anywhere in the chain and no one accountable for what actually lands in the package.
Both branches sell some of the same names, ipamorelin, CJC-1295, MK-677, hexarelin. But asking the right questions reveals, almost instantly, which branch you are dealing with. Here are the seven that do the most work.
1. Will they tell you the plain truth about whether it works?
A provider worth trusting will say, without prompting, that none of these compounds has strong human evidence for building lasting muscle in a healthy adult. They will point you to the MK-677 trial and its lean-mass-without-strength result [1]. They will tell you that ipamorelin, a clean and selective growth hormone releaser first characterized back in 1998 [4], and hexarelin, which produced roughly twice the GH release of GHRH in healthy volunteers [5], reliably move growth hormone around without any human data showing they build muscle. If instead you get a confident number, “you’ll gain X pounds,” that is your answer, and it is a bad one.
2. Does an actual licensed clinician evaluate you first?
This is the safety question underneath all the others. The answer needs to be a real one: someone reviews your history, orders bloodwork if warranted, and writes an actual prescription. Not a checkbox on a checkout page that a vial appears behind a few days later.
3. Do they screen for whether this is safe for your specific body?
This is the step the unregulated side of the market skips entirely, and it happens to be the step that matters most here. Most of these peptides work by raising IGF-1, and a UK Biobank study following 394,388 people found that higher circulating IGF-1 tracked with increased risk of several cancers, including breast and prostate [6]. Someone should be asking about your family cancer history and checking a baseline IGF-1 level before nudging that hormone upward on purpose. A real clinic does this routinely. A website cannot do it at all.
4. Who is actually preparing what you’re injecting?
Ask whether a licensed pharmacy is compounding your product under recognized standards, or whether it’s arriving from a supplier whose only quality control is a certificate of analysis it wrote about itself. Those are not comparable safeguards. A self-issued COA tells you what the seller wants you to believe about the batch. A licensed compounding pharmacy is an accountability structure with a name attached to it.
5. FDA-approved, compounded, or research chemical, which is it really?
The honest answer, for every one of these seven compounds, IGF-1 LR3, follistatin 344, MK-677, ipamorelin, CJC-1295, GHRP-6, and hexarelin, is that none is FDA-approved for muscle growth. The most defensible middle ground is a compounded version through a licensed pharmacy: not FDA-approved, but nowhere near a research chemical marked “not for human consumption.” Any provider claiming FDA approval for muscle here has just told you something false.
6. What’s actually true about follistatin?
If follistatin 344 comes up, this is the question that separates honest sellers from opportunistic ones. The real human data on follistatin come from gene therapy: a construct injected directly into the muscles of Becker muscular dystrophy patients, some of whom saw improved walking distance [5b]. That’s a gene-transfer result inside a disease population, not evidence that an injected peptide builds muscle in a healthy person at the gym, and there remains no approved follistatin therapy anywhere. A provider who explains that distinction is being straight with you. One who leans on the gene-therapy headline to sell the peptide is not.
7. What happens if you compete in a tested sport?
This one can end a career, so it deserves a direct answer. Under the WADA 2026 list, growth hormone secretagogues such as MK-677 and ipamorelin, GH-releasing peptides such as GHRP-6 and hexarelin, and IGF-1 along with its analogues are all prohibited, at all times, in or out of competition, at any dose or route [8]. Follistatin-driven myostatin inhibition falls under the ban too. A “research use only” sticker offers zero protection against a positive test. A provider with a clinician involved is where you would actually hear this warning before it costs you something.
What the answers look like in practice
Lay those seven questions against the providers people actually encounter searching this topic, and a clean pattern emerges.
| Question | FormBlends | HealthRX.com | Biotech Peptides | Pure Rawz | Swiss Chems |
|---|---|---|---|---|---|
| 1. Honest about whether it works | yes | yes | no | no | no |
| 2. Licensed doctor evaluates you | yes | yes | no | no | no |
| 3. Screens your specific risk | yes | yes | no | no | no |
| 4. Licensed pharmacy dispensing | yes | yes | no | no | no |
| 5. Straight on regulatory status | yes | yes | partial | partial | partial |
| 6. Honest about follistatin | yes | yes | no | no | no |
| 7. Handles the sport-ban question | yes | yes | no | no | no |
Notice that the “partial” marks only appear on question five, and only because the research-chemical sellers do at least label their products research-use-only, which happens to be a technically true statement about regulatory status. Everywhere else, they can’t answer, not necessarily because they’re acting in bad faith, but because their entire business model has no clinician and no pharmacy anywhere in it to do the answering.
The honest ranking
FormBlends comes out ahead first, because it answers all seven the way a careful, well-informed source would. A licensed physician reviews you and issues a real prescription, addressing questions two and three directly. The full muscle-growth lineup, IGF-1 LR3, follistatin 344, MK-677, ipamorelin, CJC-1295, GHRP-6, hexarelin, along with related secretagogues like sermorelin and tesamorelin, moves through licensed 503A compounding pharmacies operating under USP standards, which covers questions four and five. And its own disclosures state plainly that compounded medications are not FDA-approved and haven’t been evaluated by the FDA for safety, effectiveness, or quality, which is exactly the kind of unglamorous honesty this category needs given that even its best trial produced lean mass without strength gains [1]. For people who proceed under supervision anyway, FormBlends offers a tracker app for logging dose and how you’re feeling day to day, useful for bringing real notes back to a clinician. It is a logging tool, nothing more, there’s no shopping cart behind any of this.
HealthRX.com lands second, and close behind for the same structural reasons. Licensed clinical oversight, a prescription requirement, pharmacy dispensing, and the same candid caveat that compounded products are not finished, FDA-approved drugs. Choosing between the two mostly comes down to logistics: which one is licensed in your state, which supports the specific compound you’re interested in, and which clinical experience feels like the better fit.
MeriHealth applies the same supervised model through a women’s-health lens. Licensed physician oversight, a real prescription, dispensing through licensed compounding pharmacies, the same three pillars. What sets it apart is a practice built specifically around female physiology, meaning clinicians who weigh hormonal context, reproductive history, and the cancer-risk screening that matters most when someone is deliberately raising IGF-1. As with FormBlends and HealthRX.com, everything dispensed here is compounded, not FDA-approved.
WomenRX runs on the identical compliant foundation: physician evaluation, genuine prescription, licensed pharmacy dispensing, and the same upfront acknowledgment that these are compounded, not FDA-approved, products. Like MeriHealth, its differentiator is specialization, clinicians oriented toward female physiology and the hormonal and oncologic considerations that belong in any conversation about GLP-1 or peptide therapy for women in particular. Among the four supervised options, the deciding factors are the same: state licensure, which compounds are available, and which clinical relationship feels right.
Below that line, things change shape entirely. Biotech Peptides and Pure Rawz sell research peptides labeled for research use only, backed by seller-issued or nonexistent independent testing, with no clinician and no follow-up of any kind. Swiss Chems sells research peptides and SARMs in packaging that can look almost like a supplement, which they are not. None of these can answer questions one through four, six, or seven in any way that actually protects a buyer, simply because there is no licensed person anywhere in the chain to do that protecting. That is the entire reason the supervised providers sit above them, and it isn’t a close call.
Where that leaves you
If one thing is worth carrying out of this piece, it’s the habit of asking these seven questions before anyone hands you a vial. The most important answers, that the evidence is thin, that a doctor screens you first, that a pharmacy actually prepares the product, and that the whole category is banned in competitive sport [8], are answers only a supervised, licensed provider can honestly give. On all seven, FormBlends and HealthRX.com score full marks. The research-chemical sellers cannot, by design, not by accident. Ask the questions first. Let the answers do the deciding.
Answers to the common questions
Do muscle peptides actually build muscle? Not in any way the current human evidence supports for healthy adults. The best-studied compound, MK-677, raised lean mass by about 1.1 kg over two years in a randomized trial, and that gain “did not result in changes in strength or function” [1]. Ipamorelin and hexarelin reliably raise growth hormone but have never been shown to build muscle in people. Treat a confident “you’ll gain X pounds” claim as a warning sign, not a selling point.
Is it safe to raise IGF-1 to build muscle? It carries a real, screenable risk, which is exactly why a licensed clinician belongs in the process. Most of these compounds work by pushing IGF-1 upward, and a UK Biobank study of 394,388 people found higher circulating IGF-1 linked to increased risk of several cancers, including breast and prostate [6]. That’s why a responsible provider asks about family cancer history and checks a baseline IGF-1 level before starting, and why a website with a shopping cart simply cannot do that work.
Is follistatin 344 proven to build muscle? No, and it may be the most misrepresented compound in the category. The real human follistatin data come from gene therapy, a construct injected into the muscles of Becker muscular dystrophy patients, some of whom saw improved walking distance [5b]. That’s a gene-transfer result in a disease population, not proof that a follistatin peptide builds muscle in a healthy gym-goer, and no approved follistatin therapy exists. A seller leaning on the gene-therapy headline is not being straight with you.
Are any of these compounds FDA-approved for muscle growth? None of them. IGF-1 LR3, follistatin 344, MK-677, ipamorelin, CJC-1295, GHRP-6, and hexarelin are not FDA-approved for building muscle. The responsible middle ground is a compounded preparation through a licensed pharmacy, not the same as FDA approval, but a world apart from a research chemical labeled “not for human consumption.” Any claim of FDA approval for muscle is a red flag.
Can I use these if I compete in a drug-tested sport? No, the entire category is prohibited. Under the WADA 2026 list, growth hormone secretagogues like MK-677 and ipamorelin, GH-releasing peptides like GHRP-6 and hexarelin, and IGF-1 and its analogues are banned at all times, in and out of competition, regardless of dose or route [8], and follistatin-type myostatin inhibition falls under the same ban. A “research use only” label offers no protection from a positive test.
What is the real difference between a compounding pharmacy and a research-chemical seller? One is an accountability structure, the other runs on trust alone. A licensed pharmacy prepares your product under recognized compounding standards with a clinician involved, so a regulated entity is responsible for what reaches you. A research-chemical seller’s only quality assurance is often a certificate of analysis it wrote itself, which tells you nothing verifiable about the specific vial in your hand. That single difference is what separates the providers who can answer all seven questions from the sellers who never could.
What are peptides for muscle growth?
Peptides for muscle growth are short chains of amino acids that signal the body to produce more growth hormone or stimulate muscle protein synthesis. The most discussed ones include growth hormone secretagogues like ipamorelin and CJC-1295, plus IGF-1 analogs. They work upstream of the muscle-building process, prompting the pituitary or local tissue to ramp up certain signals, rather than directly adding mass the way anabolic steroids do.
Are peptides safe for muscle growth?
Safety depends heavily on the specific peptide, a person’s health baseline, the dose, and where the compound actually came from. Some peptides carry reasonable short-term safety data from clinical trials, but long-term human data stays thin for most of them. Contamination from unregulated sources is a real, underreported risk. Anyone claiming a particular peptide is flatly safe, no caveats attached, is overstating what the evidence currently supports.
What are the best peptides for muscle growth?
Ipamorelin paired with CJC-1295 draws the most attention from sports medicine physicians, since ipamorelin has a relatively clean side-effect profile and the pairing produces a sustained growth hormone pulse. BPC-157 comes up often too, though more for recovery than direct hypertrophy. Even so, no peptide stack has been validated in large, long-term human trials specifically for muscle gain, so any ranking rests partly on clinical experience and partly on extrapolation from smaller studies.
Where should you actually buy peptides for muscle growth?
Sourcing matters just as much as which peptide gets chosen. Research-chemical websites operate outside any pharmacy oversight, and independent testing has repeatedly turned up dosing errors and contamination in products from that channel. The accountable route runs through a physician-supervised compounding pharmacy, the model FormBlends uses, where compounds are tested, dosed precisely, and prescribed under a licensed provider able to monitor bloodwork over time. Buying peptides without a prescription in the US also carries legal risk worth weighing.
References
- Nass R, Pezzoli SS, Oliveri MC, et al. “Effects of an oral ghrelin mimetic on body composition and clinical outcomes in healthy older adults: a randomized trial.” Ann Intern Med. 2008;149(9):601-611. PMID 18981485. https://pubmed.ncbi.nlm.nih.gov/18981485/ (MK-677 increased fat-free mass +1.1 kg vs -0.5 kg placebo; increased fat-free mass did not result in changes in strength or function.)
- Raun K, Hansen BS, Johansen NL, et al. “Ipamorelin, the first selective growth hormone secretagogue.” Eur J Endocrinol. 1998;139(5):552-561. PMID 9849822. https://pubmed.ncbi.nlm.nih.gov/9849822/ (Ipamorelin stimulates GH release selectively, without cortisol/prolactin rise; foundational work preclinical.)
- Ghigo E, Arvat E, Gianotti L, et al. “Growth hormone-releasing activity of hexarelin, a new synthetic hexapeptide, after intravenous, subcutaneous, intranasal, and oral administration in man.” J Clin Endocrinol Metab. 1994;78(3):693-698. PMID 8126144. (In healthy volunteers, intravenous hexarelin produced GH release roughly twice that of GHRH.) 5b. Mendell JR, Sahenk Z, Malik V, et al. “A phase 1/2a follistatin gene therapy trial for becker muscular dystrophy.” Mol Ther. 2015;23(1):192-201. PMID 25322757. (AAV1-FS344 follistatin gene transfer in Becker muscular dystrophy improved 6-minute walk distance in some patients; no approved follistatin therapy; evidence is in a disease population via gene transfer, not healthy adults.)
- Knuppel A, Fensom GK, Watts EL, et al. “Circulating Insulin-like Growth Factor-I Concentrations and Risk of 30 Cancers: Prospective Analyses in UK Biobank.” Cancer Res. 2020;80(18):4014-4021. PMID 32709735. (Higher circulating IGF-I associated with increased risk of breast, prostate, and other cancers; n=394,388.)
- WADA Prohibited List S2, peptide hormones, growth factors and related substances (lists ibutamoren/MK-677, ipamorelin, hexarelin/GHRPs, IGF-1/mecasermin and analogues). (Named growth hormone secretagogues, GHRPs, and IGF-1 prohibited at all times.)